What Is Hypopharynx Cancer?
A type of throat cancer known as hypopharyngeal cancer develops in the hypopharynx or lower region of the throat. When cells develop abnormally, grow out of control, and have the ability to spread to other body areas, cancer results. A mass or lump is created when these cells accumulate.
The piriform sinuses, which are pockets on either side of the hypopharynx, are frequently the site of hypopharyngeal cancer. Squamous cell carcinomas, which originate from the cells lining the inside of the throat, account for the majority of hypopharyngeal cancers.
What is hypopharynx?
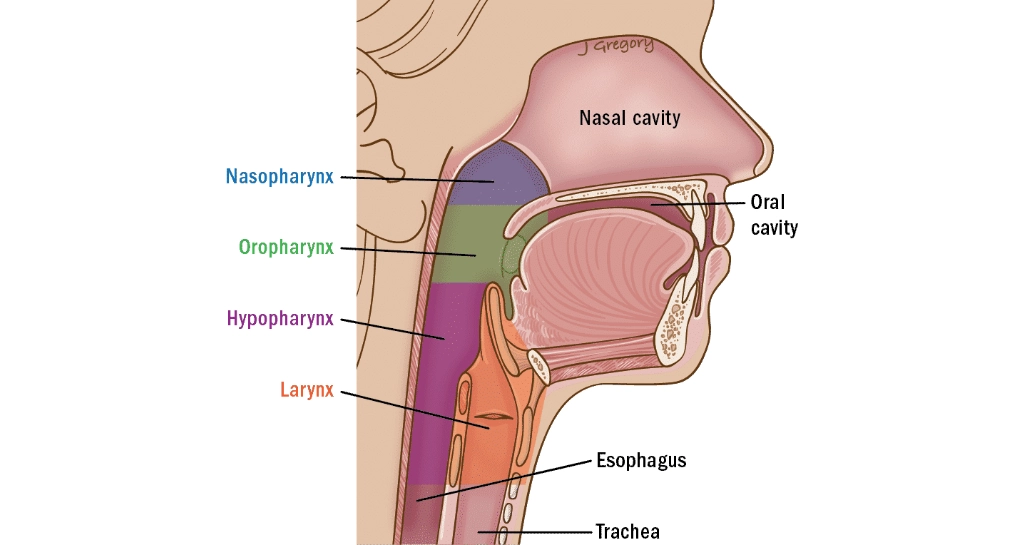
Pharynx is the medical term for the throat and is divided into 3 parts:
- Nasopharynx: the area behind and above the nose.
- Oropharynx (the tonsils and mid-throat region)
- Hypopharynx, or the throat below
The oesophagus, commonly referred to as the gullet, is situated behind the larynx (voice box), and it is connected to the hypopharynx, the lowest section of the throat.
Signs and Symptoms of the Hypopharynx Cancer
The location, size, and extent of the disease’s dissemination inside the body determine the signs and symptoms of hypopharyngeal carcinoma.
Some individuals with hypopharyngeal cancer can have no symptoms at all.
Typical indications and manifestations include:
- Voice raspiness
- Discomfort during swallowing, such as a painful throat or ear pain, especially on one side
- A lump in the throat caused by enlarged glands or lymph nodes.
- Breathing loudly or difficultly
See your physician as soon as possible if any of these symptoms persist for longer than a few weeks. They might be able to assist with your diagnosis and care.
Tests for Hypopharynx cancer
It’s critical that your physician confirms the diagnosis of hypopharyngeal cancer, evaluates the disease’s extent, and determines whether it has progressed to the body’s lymph nodes in the neck or elsewhere.
Your doctor will need to do the following tasks to respond to these inquiries:
- Discuss your medical history with you. This covers any symptoms you may have observed, any medical issues you may have, any medications you take, and if you smoke or consume alcohol.
- Conduct a physical examination that includes checking and touching inside your neck and throat and ordering any necessary diagnostic procedures, such as scans.
- Not everyone will require It is not necessary for everyone to get every test for hypopharyngeal cancer. Appropriate tests for you will be recommended by your physician.
The most popular tests for cancer of the hypopharynx are:
- Autopsy
- Blood Examinations
- Computed Tomography, or CT Nasoendoscopy scan
- Magnetic Resonance Imaging or MRI Positron Emission Tomography (PET) scan Scan with Ultrasound
Options for Hypopharyngeal Cancer Treatment
For hypopharyngeal cancer, there are three possible courses of treatment:
- Surgery: A variety of procedures are available for the removal of hypopharyngeal cancer.
- Radiation therapy: Radiation therapy may be necessary for certain patients with big or advanced hypopharyngeal cancer after surgery.
- Chemoradiation: Often known as radiation treatment administered in conjunction with chemotherapy, can be performed with or without surgery.
1. Surgery for Hypopharynx Cancer
The following are the many surgical options for hypopharyngeal cancer:
- Laser Transoral Microsurgery
- The hypopharyngectomy
- Tracheopharyngectomy
- Dissection of the Neck
- Surgery for Reconstruction
- Tracheostomy
2. Radiation Therapy
Radiation therapy with feeding tubes for hypopharyngeal cancer
External beam radiation is the most often used radiation therapy method for hypopharyngeal cancer. External radiation is used in this kind of radiation therapy.
Radiation therapy has the following applications:
Definitive
This is a viable therapeutic option for patients suffering from hypopharyngeal cancer. Preserving the larynx and its function is the goal of this treatment. It is a substitute for surgery, which could entail a laryngectomy, or removal of the voice box. Radiation therapy is a complete treatment for hypopharyngeal cancer, including surrounding tissue and lymph nodes on both sides of the neck. Radiation therapy is administered seven days a week (with no treatment on weekends) and can be administered as follows:
- Only definitive radiation therapy
- Either definite radiation therapy by itself, or definitive radiation therapy in conjunction with concurrent chemotherapy, which increases the efficacy of radiation therapy by adding chemotherapy.
Adjuvant
At this point, radiation therapy is administered following the hypopharyngeal cancer’s surgical excision. Adjuvant radiation therapy is used as a follow-up treatment to eradicate cancer cells that may have remained in the lymph nodes on both sides of the neck and in the hypopharynx after surgery. To allow for surgical healing, it typically begins four weeks following surgery. A course of radiation therapy typically lasts six weeks. Adjuvant radiation therapy, often known as chemoradiation, can occasionally be enhanced by the use of chemotherapy.
Palliative
Another use for palliative radiation therapy is to treat the symptoms of Additionally, palliative radiation therapy is utilised to treat advanced hypopharyngeal cancer symptoms. Palliative radiation therapy may be necessary for symptoms such as pain, bleeding, difficulty breathing, and difficulty swallowing.
3. Chemotherapy for Hypopharynx Cancer
Chemotherapy acts by causing harm or death to cancer cells. It is often injected into a vein using a needle that has a cannula (tube) connected for hypopharyngeal cancer.
Chemotherapy can be applied in a variety of methods to treat hypopharyngeal cancer, such as:
Definitive
Chemoradiation, or chemotherapy plus radiation therapy, is sometimes used. Usually, advanced-stage hypopharyngeal malignancies are treated with it. This can be administered once every three weeks or once a week during the course of radiation treatment. Chemotherapy increases the effectiveness of radiation therapy in eliminating cancer cells, but most patients experience additional side effects as a result.
Adjuvant
This is the situation in which radiation therapy and chemotherapy are administered following surgery (chemoradiation). This can be administered every day that radiation therapy is administered, once every three weeks, or once a week. Chemotherapy increases the effectiveness of radiation therapy in eliminating cancer cells, but most patients experience additional side effects as a result.
Neo- Adjuvant
In order to assist decrease big malignancies and make them easier to remove during surgery or target with radiation therapy, chemotherapy is sometimes administered prior to radiation therapy or surgery.
Palliative
When cancer is incurable, this is employed. Surgery may not be an option because the cancer is too big or has spread too far. Palliative chemotherapy aids in symptom relief and slows the spread of cancer.
Your medical oncologist will select one or more chemotherapy drugs based on which ones are most appropriate for your particular type of cancer before you begin treatment.
Your doctor’s selection of chemotherapy drugs may be based on:
- The treatment’s intended outcome
- Curative or palliative
- Your medical history
Adverse Reactions to Chemotherapy
Chemotherapy side effects are contingent upon the medication used and the dosage prescribed by your physician. The three most often prescribed drugs are cetuximab, carboplatin, and cisplatin.
Chemotherapy has varying effects on various people. While some people could have a few adverse effects, others might not react differently to treatment. While some individuals might encounter a few adverse effects, others might not have any at all. Common adverse effects of chemotherapy include the following:
Feeling like you want to throw up (nausea) or experiencing more vomiting side effects from radiation therapy. Most of these side effects are transient and may go away after your chemotherapy treatment is over. Certain adverse effects may not go away for months or years, or they may be irreversible.
You will have routine follow-up appointments after radiation therapy to allow your doctor to assess your progress, ensure that the cancer has not returned, and monitor and manage any side effects you may be experiencing.
Your physician can advise that you have some particular supportive treatment.
- Renal damage brought on by certain drugs
- Hearing loss or weakening auditory nerve
- Increased risk of infection due to rash (if the chemotherapy lowers the blood’s white cell count)